- Also see my second Feb. 17 post here, and my third post on Feb. 19 here where I commented on HisTalk's take on these issues.
Feb. 13: I have observed unseemly things about health IT in my nearly two decades in medical informatics. For example, my dealings with health IT vendor HBOC (no relation to HBO and now merged into McKesson) whose erstwhile CEO was cooking the books, and a-little-too-cozy relationships between hospital CIO's and health IT vendor CEO's.
Even considering those observations, the matter below is quite unsettling if its allegations are valid. It is additionally unsettling considering the many well-intentioned volunteers who give of their time in CCHIT activities, whose reputations might be unfairly tarnished if there are significant undisclosed problems. (I applied to be a volunteer some years ago, in fact, but was not selected initially, and did not reapply due to my work schedule).
Seen at the WSJ Health Blog
here about the
CCHIT (
Certification Commission for Healthcare Information Technology) is the post below. An involuntarily dissolved organization? Conflicts of interest with
HIMSS, the Healthcare Information and Management Systems Society (a healthcare IT vendor alliance), and other "front" organizations?
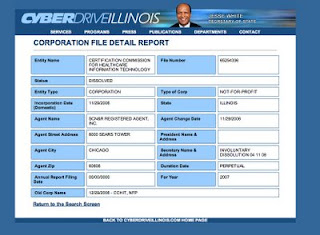
I do not know who posted this series of allegations, and importantly do not represent them as true; they may be rumors, misinformation, politically motivated or statements of disgruntled individual(s). However, I checked one of the allegations and verified it. I utilized Illinois' online corporation/LLC search utility at
http://www.ilsos.gov/corporatellc/CorporateLlcController and did indeed find this puzzling entry for CCHIT as "involuntarily dissolved" on 4/11/2008. I could not find other entries even under the full name "Certification Commission for Healthcare Information Technology."
Here is the results screen (click to enlarge):
 Edgar online company search
Edgar online company search finds no company listings for "CCHIT" or "Certification Commission for Healthcare Information Technology", either.
Another private nonprofit lookup of unknown reliability, Melissadata.com, shows CCHIT as a 501 (c)(3) in Chicago listed as "exempt" from taxes since October 2008, last 990 form ("
Return of Organization Exempt from Income Tax") filed Dec. 2007, form 990 amount $4,740,146, as shown
here. This would have been before the involuntary dissolution. No 2008 form 990 data is shown.
A number of reasons for
involuntary dissolution of a nonprofit in one state can be seen
here.
This certainly raise concerns and questions such as:
- Why was this not for profit "involuntarily dissolved" in April 2008? For what reason(s)?
- By whom?
- What replaced it?
- Why was this dissolution not widely known?
- What is CCHIT now? Is the Illinois online corporation/LLC database faulty? Does it remain a non-profit?
- If the Illinois database is not faulty, where is CCHIT now registered? Is it registered?
- Is it a subsidiary of HIMSS or other organization?
- Where do CCHIT monies go?
- Who controls the funds?
- Who assures that it is indeed impartial in its assessments?
The posted comment at the WSJ health blog that caught my attention reads (emphases mine):
Why not pack CCHIT EHR certifications in Cracker Jack Boxes? If folks think CCHIT is a real organization and the certification is anything more then a stamp of approval from the HIMSS Circus they need to think again after looking at the facts.
Some facts are known about the Certification Commission for Health Information Technology. The Certification Commission for Health Information Technology (CCHIT) is a defunct Illinois Not-For-Profit 501(c) 3, which operates to take money from the Office of the National Coordinator and Vendors by offering to sell a “Certification”.
DID I say DEFUNCT? Yes I said DEFUNCT…please read on.
The Not-For-Profit 501(c) 3, Certification Commission for Health Information Technology (CCHIT), operates a “Front” office located at 200 S. Wacker Drive, Chicago, Illinois.
CCHIT, as it is known, represents itself as a government recognized organization for certifying electronic health records. CCHIT has received monies from the United States Government (estimated over $2.5 million to date) and monies from vendors of electronic health records.
CCHIT was formed as a NFP in the State of Illinois and is an entity spawned by none other, HIMSS.org. CCHIT is no longer a legal entity existing within the State of Illinois effective April 11, 2008, but continues to engage business as a 501(c) 3 accepting payments as reported by J. Morrisey, Director of CCHIT Communications (February 3, 2009).
CCHIT continues to hold itself out to take money for the sale of “Certification” (a rubber stamp device the buyer can display on his product if the fee is paid), a contrived performance standards product label developed by its parent organization, Healthcare Information and Management Systems Society (HIMSS), a lobbyist, with headquarters at 230 E. Ohio St., Chicago, Illinois.
CCHIT was also located within the HIMSS Headquarters at 230 E. Ohio Street in Chicago but moved to Wacker Drive apparently due to appearances of being too close to the lobbyist parent organization.
CCHIT, through the organization that spawned them—HIMSS.org, a lobbyist organization—recently asked for $25 Billion additional funds in an open letter to the Obama administration (http://www.himss.org/advocacy/). HIMSS, through its agent H. Stephen Lieber, provided CCHT with $300,000 seed money in 2006 with which to fund a startup operation.
HIMSS receives money from CCHIT as a subcontractor, as the payoff for seeding the startup. HIMSS provides public commentary through the use of its own members for certification criteria back to CCHIT. HIMSS is also the parent company for the Electronics Health Record Vendor Association (EHRVA), another Not-For-Profit housed at 230 E. Ohio St., Chicago, Illinois.
The Facts:
1. The Chairman of CCHIT is Mark Leavitt, MD, PhD. Mark Leavitt is also Chief Medical Officer with HIMSS.org. It is believed Mark Leavitt may be a relative of Mike Leavitt, former HHS Secretary [doubtful - ed.]
2. CCHIT takes federal money, and money from vendors, in exchange for the sale of “certification”. CCHIT does not have a legitimate physical address where it conducts its testing. CCHIT has a “front” office at 200 S. Wacker Drive, Chicago, Illinois, with previous headquarters at 230 E. Ohio St., Chicago, Illinois. CCHIT is, in fact, now defunct.
3. CCHIT has no legitimate registration certificate of good standing with the State of Illinois, the state in which it is purportedly chartered as a 501(c) 3. It is, in fact, listed as “involuntarily dissolved” effective April 11, 2008, file# 65254336. Illinois State listing here: http://www.ilsos.gov/corporatellc/
4. CCHIT does not provide independent inspections of its facility or 3rd party reviews of its findings. “Certification” status of vendor products granted by CCHIT after the Illinois State’s involuntary dissolution date of April 11, 2008 appears to be without merit or bogus, and CCHIT operates deceptively to convey legitimacy.
5. CCHIT operates fraudulently within the State of Illinois and in the United States to take money from vendors of electronic health record systems and from taxpayers; the CCHIT business practice presents as a Pay-For-Play scheme; if the vendor pays, CCHIT certifies the product conveying a competitive advantage in the marketplace. There is no transparent certification testing for 3rd party review. The costs to certify are in the many tens of thousands per vendor. Officers and Directors of CCHIT have taken money in exchange for “Certification“, knowing its 501(c) 3 operational status to be defunct.
6. CCHIT, a dissolved entity and defunct 501(c) 3 Not-For-Profit, receives funding from the Office of the National Coordinator (ONCHIT) and is tied to a lobbyist organization that claims to be a Not-For-Profit, HIMSS.org—the organization that spawned CCHIT and which formerly housed the entity in its corporate headquarters located at 230 E. Ohio St., Chicago, Illinois. Why does CCHIT continue to certify vendor products when its own corporation has been involuntarily dissolved? Does the word “MONEY” ring a bell?
CCHIT continues to hold itself out as a certifying entity when it can’t even certify to the state of its incorporation that it does in fact exist.
Closing thoughts:
The certification process and testing should be reviewed carefully, and those vendor companies whose products were certified after CCHIT’s involuntary dissolution should be contacted. Money should be returned to the vendors and the taxpayers- CCHIT is a bogus operation.
CCHIT should NOT be allowed to receive future Federal grants and monies from the United States Government as part of the stimulus package. CCHIT is defunct, moreover the cozy relationships between CCHIT, ONC, CMS, HITSP and others are bankrolled with taxpayer money and money from HIMSS.org and its others.
Through all the smoke and mirrors we the people are supposed to trust these [derogatory term redacted - ed.] and they actually think we are buying it?
There is no point in CCHIT holding itself out as a legitimate entity at HIMSS Annual Conference either, CCHIT is a defunct organization and has been since the beginning of 2008…DUH!
CCHIT has flown under the radar for a year and a half, the jig is up and the whistle has been blown.
CJ
Comment by cj - February 13, 2009 at 2:10 am
I find these allegations potentially very troubling regarding an organization that is supposed to be "impartial" and a judge of the suitability of electronic health records products for sale here in the U.S. The answers may be simple and straightforward. I hope they are. Healthcare IT already has
significant problems and needs no more.
These are important issues worthy of clarification. I would welcome clarifications from CCHIT, which I will certainly publish here.
-- SS
Addendum Feb. 15:
I note the
following response at the WSJ blog:
The “facts” in the previous post are deliberate misinformation from an anonymous source.
1. Mark Leavitt, chair of the Commission, is not employed by HIMSS as CMO nor is he a relative of Mike Leavitt, previous Sec. of HHS.
2. CCHIT conducts jury-observed and technical testing of vendor-submitted products, requiring that the products meet 100% of the compliance criteria published at http://www.cchit.org/certify/index.asp. It’s current administrative offices are at 200 S. Wacker Drive, Suite 3100, Chicago, Illinois.
3. CCHIT was founded originally as a LLC but has subsequently transitioned to a private, nonprofit 501(c)3 organization. That is its current status.
4. CCHIT operates with the oversight of both its board of trustees - managing its business functions - and board of commissioners, which provides oversight of its certification development programs and inspection processes.
5. CCHIT’s trustees and commissioners receive no compensation; they serve in a volunteer capacity. CCHIT operates with a paid staff of about 20 personnel who support the work of the Commission and it’s 15 volunteer work groups, administer the certification inpections and provide outreach to its diverse stakeholders
6. CCHIT now operates independently of HIMSS, AHIMA and NAHIT - its founding organizations - and no money provided by ONC for developent or by vendors for the conduction of inspections is returned to those organizations.
Any questions about CCHIT’s operations may be directed to me at the following email address.
Sue Reber, Marketing Director
CCHIT
sreber@cchit.org
This still does not explain the involuntary dissolution nor the absence of an "active" entry in the Illinois' online corporation/LLC search utility. I have sent Ms. Reber an initial inquiry.
It also does not explain possible conflict of interest concerns. If CCHIT operates independently of HIMSS, AHIMA, and NAHIT, why are individuals from some of these organizations acting as
Trustees? Why are vendor officials acting as
Commissioners?
Organizations such as the
ECRI Institute, that independently evaluates medical technologies, seems to have a credible approach to avoid appearances of conflict:
The Integrity of Independence
Our conflict-of-interest rules have been carefully developed to create an environment that maximizes objectivity, productivity, and integrity of process. We accept no advertising revenues from any source. Our employees are not permitted to own stock shares in medical device or pharmaceutical firms, and we verify this by examining each employee’s federal income tax return. We go beyond the industry norm to ensure that you receive unbiased guidance.
-- SS
(also see my Feb. 17 follow up post here.)




{kind=link}